Masks (non-N95) protects you only 1 percent (1%) of the times, CDC said in 2018
As coronavirus continues to spread around the world, there is a growing demand for face masks as people look for ways to protect themselves from the deadly virus. But this raises the question millions of people have been asking is: Do face masks actually work? The quick answer is: Yes, face masks do provide varying levels of protection. However, more research is needed about the effectiveness of masks in controlling the spread of COVID-19.
To date, there is no conclusive study that shows masks are 100% effective. In fact, the World Health Organisation (WHO) and the CDC, have shifted their position multiple times on whether people should wear masks since the pandemic started 9 months ago. At one point, WHO said people don’t need the virus unless they’re sick. These shifting guidelines further sowed confusion as to the effectiveness and benefits of masks. The jury is still out on the science and effectiveness of masks.
Early this week, we wrote a story about the Centers for Disease Control and Prevention (CDC) after the agency published a study that showed 85% of COVID-19 cases were people who often or always wear masks. The CDC study, which was released in September, looked at the behavior of these 314 symptomatic people who sought out testing at 11 particular sites in July. According to the CDC guidance on masks, wearing a mask is intended to protect other people in case the mask wearer is infected.
However, a 2018 study published by the CDC raises some doubts about the effectiveness of surgical masks, which we all know provide better protection than the regular cloth masks. In the article titled, “Non-occupational Uses of Respiratory Protection – What Public Health Organizations and Users Need to Know,” CDC said, “that on average only 1% of the times that a surgical mask was put on (range: 0% to 7% across 6 models) resulted in adequate levels of protection.”
“However, members of the general public wearing loose-fitting facemasks and improvised devices rarely approach the level of protection found by respirator wearers. For example, one study found that on average only 1% of the times that a surgical mask was put on (range: 0% to 7% across 6 models) resulted in adequate levels of protection. This is not surprising as loose-fitting facemasks and improvised devices are not designed to seal tightly to the face and thus cannot prevent particles in the air from bypassing the filter and being drawn into the respiratory tract during normal breathing.”
Just to be clear, a surgical mask, also called a medical mask, is a loose-fitting disposable mask that protects the wearer’s nose and mouth from contact with droplets, splashes, and sprays that may contain germs. A surgical mask also filters out large particles in the air and may protect people by reducing exposure to the saliva and respiratory secretions of the mask wearer.
Surgical masks should not be confused with N95 mask. The N95 mask is actually a type of respirator that offers more protection than a surgical mask does because it can filter out both large and small particles when the wearer inhales. As the name implies, the N95 mask is designed to block 95% of very small particles.
CDC went on to say that “improvised devices such as bandanas and t-shirts, non-NIOSH-approved single-strap dust masks, and loose-fitting facemasks will not provide the same level of protection as a NIOSH-certified respirator.” NOISH stands for National Institute for Occupational Safety and Health.
Not sure why this article is not making the news. Just a few weeks ago, CDC Director Robert Redfield made a contradictory claim saying surgical masks offered more protection than a vaccine. “I might even go so far as to say that this face mask is more guaranteed to protect me against Covid than when I take a COVID vaccine,” Redfield said. He later walked back his comments. A couple of hours after his briefing to the Senate, Dr. Redfield went on Twitter to express his commitment to vaccines. “I 100% believe in the importance of vaccines and the importance in particular of a #COVID19 vaccine. A COVID-19 vaccine is the thing that will get Americans back to normal everyday life,” Dr. Redfield said in a Twitter post.
The question we might want to ask is, what do other scientists think about masks? For that, we turn a chemist and an experienced expert in personal protective equipment (PPE), Roger W. Koops holds a Ph.D. in Chemistry from the University of California. Dr. Koops worked in the Pharmaceutical and Biotechnology Industry for over 25 years. In his article titled, “The Year of Disguises,” Dr. Koops did an excellent job in educating his readers about viruses and how masks work.
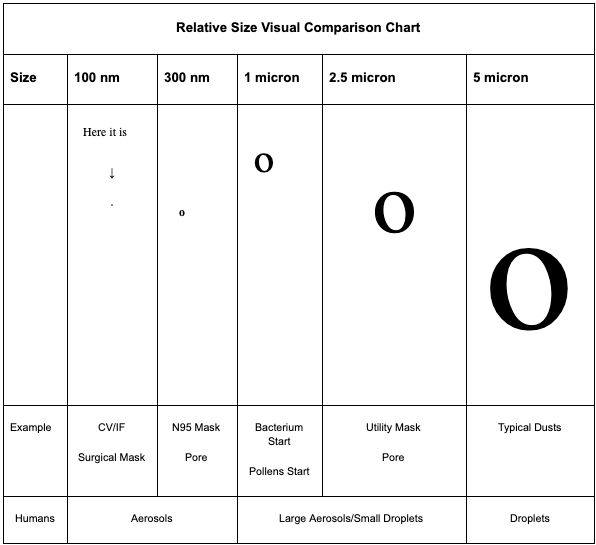
Credit: Dr. Roger W. Koops
Using this scale as a reference, Dr. Koops first clear up the confusion about the misunderstanding about what “mask” really means. Below is how he explained it.
The term “mask” by itself means nothing. It is like saying “car.” You have to identify it more specifically because there are many different types and varieties, just like cars. So, for this essay, I will use two terms as follows:
- Face Coverings: In this category I will include homemade cloth, dust, non-fitted utility, custom stylish, and any other common “mask,” i.e. something that is intended to cover your mouth and nose and that is by and large used in the general population (because they are cheap and inexpensive).
- Mask: In this category, I am referring specifically to the SURGICAL mask and N95 mask (which is recommended for use in clinical settings by health care workers). If necessary, I will specify between them.
One of the big mistakes by modelers is the concept of a face covering or mask as a “barrier.” I see many references to so-called “experts” who make this claim. This is completely false. No face covering or mask is a barrier. Either they do not know what they are talking about or they are misleading people.
Masks and “Face Coverings” ARE:
- FILTERS, not barriers. They FILTER only the things that they are designed to filter, to a level of efficiency based upon design, usually not at 100% efficiency. For example, the N95 mask is designed and rated to filter particles greater than 300 nm at 95% efficiency (note: there are masks with greater efficiency than 95%, such as the N99 and NHEPA, but these are very expensive).
- Bidirectional, or two-way street flow (unlike my respirator above). That means the air is intended to go in and out through the same place – breathe in, breathe out. The filtering ability affects both ingress and egress, but MOST are intended to be used towards ingress, i.e. to protect the wearer (Surgical masks are the exception).
- Designed for normal breathing patterns, not exertive force (although the Surgical mask has a pressure rating). This is an important point!
- NOT designed to filter infectious agents but rather inert particulates (except the Surgical mask which is intended to preserve a sterile/sanitary operating field).
- Designed for minimal usage time. They are NOT intended to be stuck on your face for hours.
Dr. Koops went on to explain what happens when after we wear masks and take them off after use. Here is what he said.
First, what happens on EGRESS. We will look at droplets because most face coverings will not stop an aerosol and the 2020 propaganda has been focused on droplets.
Assuming that a person is shedding virus and they produce droplets that contain hitchhiking virus, and assuming the face covering actually stops ALL droplets (best-case scenario), the following molecular pathway will likely occur:
- The droplet will lose its moisture. The timing may be different than just going out into the environment but moisture will be lost. However, the expelled droplets may accumulate faster than evaporation. If that happens, the facial covering starts to become saturated with moisture, mucus, cellular debris, bacteria, etc. as well as virus molecules.
- The virus molecule DOES NOT EVAPORATE and no matter what happens as far as the droplet is concerned, the virus is now on the face covering, at least initially. This means that the face covering is now contaminated and is a possible source of transmission, both contact and airborne.
- The virus is not somehow magically “glued” to the mask but can be expelled, whether or not there is still moisture. This can happen the next time a person breathes, speaks, coughs, sneezes, hisses, grunts, etc. So, the virus can be expelled out INTO THE ENVIRONMENT from the face covering.
So, the face covering acts as an intermediary in transmission. It can alter the timing of the virus getting into the environment, but it now acts as a contact source and airborne source; virus can still get into the environment. Since we know that the stability is good on most covering and mask materials, it does nothing to break down the virus until the covering is removed and either washed or discarded (appropriately).
Here is an important point, as more virus molecules accumulate, more are expelled. The face covering is not some virus black hole that sucks the virus into oblivion.
Second, what about INGRESS?
What works for egress works for ingress. So, if a person is wearing a face covering and they encounter virus, aerosols, or droplets, the virus and aerosols will likely penetrate. If the droplet is stopped, the surface is now contaminated. This means that if the surface of the covering touches the mouth or nose, you can become contaminated, i.e. infected.
This is a common sight with most face coverings, including the “stylish” coverings that people are wearing (I often see the covering moving back and forth against their mouth and nose even as they breathe, like a diaphragm), as well as with the cheaper dust masks and homemade cloth masks. If you inhale, you can become contaminated. If you touch the face covering, such as pulling it up and down, you can become contaminated.
Further, because the surface is contaminated, a person can also expel the virus back out into the environment just as with egress. This can be done by talking, breathing, coughing, etc.
Dr. Koops made the following observation:
“Stopping a *droplet* is NOT the same as stopping the virus!”
In the end, Dr. Koops concludes with the following important points for consideration:
- People who have experienced this virus do NOT need to wear face coverings, period.
- In the open environment, no one should be wearing face coverings. This is the one place where we can get an assist from nature to help reduce the virus molecules. Considering that less than 5% of transmissions have been associated with open environments (and identifiable activities not random encounters), the risk is truly small.
- A face covering may be useful when visiting an at-risk elderly person or in a controlled health care setting such as a hospital or nursing home. But, I think that these should be dispensed by trained personnel and should be focused on using Surgical masks wherever possible. The protection is not so much from viruses but face coverings may be more effective in preventing the spread of bacteria and fungi.
- Children should not be wearing face coverings. We all need constant interaction with our environments and that is especially true for children. This is how their immune system develops. They are the lowest of the low risk groups. Let them be kids and let them develop their immune systems..
- The “Mask Mandate” idea is a truly ridiculous, knee-jerk reaction and needs to be withdrawn and thrown in the waste bin of disastrous policy, along with lockdowns and school closures. You can vote for a person without blindly supporting all of their proposals!
- There may be other health risks associated with continued use of face coverings. While this is anecdotal, I have many physician acquaintances and they are all reporting increases in conditions that may be associated with face coverings, such as facial skin infections, nose/throat and sinus infections, even anxiety conditions. An area of concern is the change in breathing patterns that can be directly associated with face coverings. I train regularly. The only time that I wear a face covering is to gain entrance to the public gymnasium where I train (because it is required). The mask is discarded immediately when I start training, as most other people also do. The staff members do not make a fuss because they understand the dangers of doing exertion with a face covering.
- We also do not know enough about the possible consequences of forcing whole populations to adopt face coverings for extended periods. There may be both health and social consequences that we cannot consider at this time. Humans have developed as creatures whereby we interact with our environment. Our whole upper respiratory tract has developed immense defensive systems because of that. I am worried personally about “unnatural selection.” This is when human actions force a direction of evolution that would not otherwise occur. Often, the result is not good. But that is a whole different subject that needs to be considered.
Below is a BBC video that sheds more light on the effectiveness of masks.

